Building Resilient Psychiatric Care Systems Under Workforce Strain
How hybrid clinical models protect access, quality, and clinician sustainability
Psychiatric Care Designed for a Workforce Under Pressure
Psychiatric care today is under growing pressure. Across emergency departments, inpatient units, and community settings, health systems are struggling to keep pace with rising demand and limited psychiatric expertise. This gap is felt in tangible ways: patients wait longer during crises, clinicians manage heavier and more complex caseloads, and care teams are asked to do more with fewer resources.
This imbalance affects more than access: it compromises care quality and safety, disrupts continuity across settings, and strains the well-being of clinicians. National workforce projections suggest these challenges are not temporary. Psychiatric shortages are expected to persist and deepen, particularly in high-acuity environments where timely, specialized care is essential (Levin et al., 2024).
Many responses to this crisis focus primarily on filling coverage gaps. While necessary, coverage alone does not address the clinical and operational challenges of a sustained workforce shortage. Without intentional system design, efforts to expand access can inadvertently create fragmented care, increase clinician burnout, and produce inconsistent standards across settings, placing both patients and providers at risk (Xiong et al., 2025).
Addressing these challenges requires care models that are not only accessible, but also clinically rigorous and sustainable. Precise Clinical was created to help relieve these system-level pressures, with an emphasis on supporting patients during moments of acute need. It also seeks to protect the clinicians and care teams delivering that care, particularly in environments where demand consistently exceeds capacity.

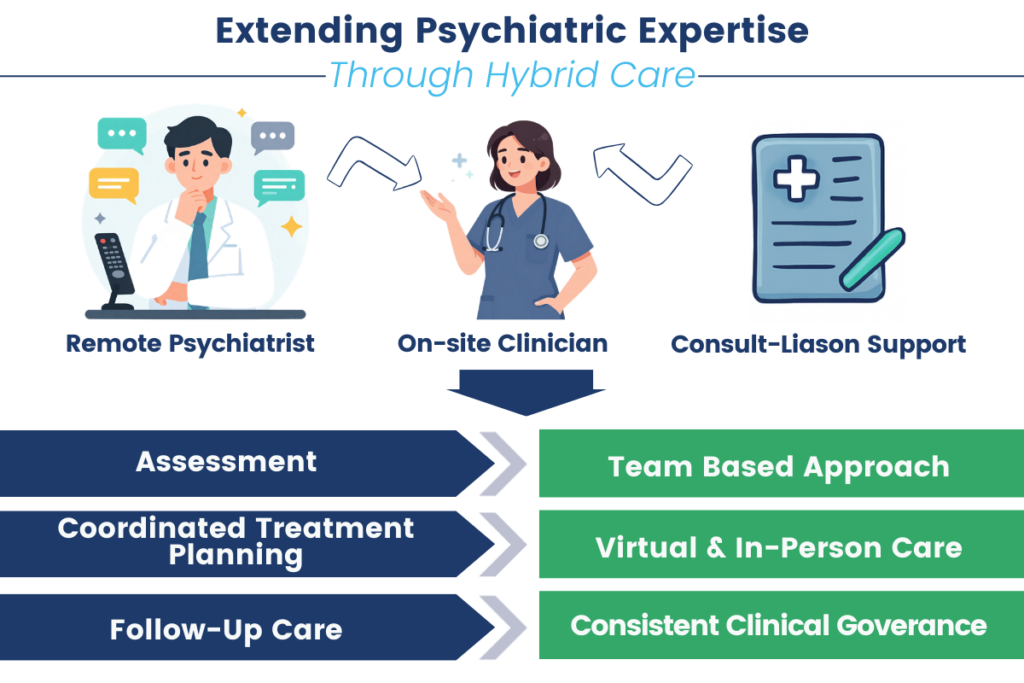
Extending Psychiatric Expertise Through Intentional Care Models
Hybrid psychiatric care models have emerged in response to these pressures. Designed to reflect how care actually unfolds in real-world settings, these models integrate in-person services with virtual and consultative support, allowing psychiatric expertise to reach patients when and where it is needed most. This approach acknowledges that no single setting or modality can meet the full range of patient needs on its own.
In effective hybrid models, virtual psychiatry functions not as a replacement for in-person care but as an extension of the clinical team. On-site clinicians, remote psychiatrists, and consult-liaison providers work within shared clinical frameworks that enable prompt evaluations, collaborative decision-making, and coordinated treatment planning. This team-based approach helps preserve clinical quality even during periods of high demand.
Evidence from collaborative care and consult-liaison models suggests that integrated approaches can expand access while maintaining consistency, oversight, and clinical integrity (Hernandez et al., 2024).
When thoughtfully implemented, hybrid models increase reach without compromising the standards of psychiatric practice.
Workforce Support as a Clinical Imperative
Workforce shortages are closely linked to clinician well-being. Persistent staffing gaps force clinicians to manage heavier workloads, handle more complex and higher-acuity cases, and recover with less time and support. Over time, this sustained pressure contributes to rising burnout, earlier departures from clinical roles, and the loss of experienced providers, further worsening existing shortage (Sipos et al., 2024).
Care models that fail to account for these realities of risk accelerating workforce attrition rather than alleviating it. Distributing clinical responsibility across teams and time, providing consultative support, and designing coverage structures that maintain accountability while reducing individual burden are essential for sustainable care.
The Precise Clinical care model acknowledges these pressures, focusing on shared responsibility and flexible support structures that help reduce strain while preserving clinical accountability.
Supporting clinician well-being is not simply an operational concern. It is a clinical imperative, fundamental to delivering safe, effective, and compassionate psychiatric care for patients.
Maintaining Continuity Across the Care Continuum
Psychiatric workforce shortages often expose the most fragile points in the behavioral health continuum. Transitions between emergency departments, inpatient units, and outpatient care are particularly vulnerable when psychiatric expertise is limited. Delays in assessment, fragmented handoffs, and poorly coordinated discharge planning increase the risk of prolonged length of stay, readmissions, and adverse patient outcomes (Aggarwal et al., 2024).
Maintaining continuity across these transitions is therefore central to both patient safety and system efficiency. Early psychiatric involvement, coordinated care planning, and structured follow-up support reduce unnecessary admissions and support safer, more timely discharges. Approaching psychiatric care as a connected system rather than a series of isolated encounters allows health systems to manage demand while preserving patient-centered outcomes.
Within the Precise Clinical framework, continuity is supported through integrated care pathways that span acute, inpatient, and post-discharge settings, ensuring that clinical decisions at one point in care are informed by and aligned with the next.
Clinical Governance as the Foundation of Quality
Expanding access without robust clinical oversight introduces significant risk. In already strained environments, inconsistent standards, unclear escalation pathways, and divided accountability can compromise both safety and quality. For this reason, clinical governance must remain central as psychiatric care models evolve.
Research on workforce shortages indicates that quality deterioration is most likely when staffing solutions lack clear clinical accountability (Gilles et al., 2025). Governance is embedded into hybrid care models through standardized assessments, structured workflows, and trauma-informed principles. This approach ensures psychiatric evaluations remain evidence-based and consistent while staying aligned with best practices across care settings.
Strong clinical governance is embedded throughout the Precise Clinical model, supporting quality and safety across modalities without limiting flexibility or access.
Quality is not an incidental outcome of scale. It is the result of deliberate, disciplined clinical design.
Building Resilient Psychiatric Care Systems
Psychiatric workforce shortages are unlikely to resolve in the near term. Addressing them requires care models that acknowledge systemic constraints while actively protecting patient safety, clinical rigor, and clinician sustainability.
Resilient systems are created through the thoughtful integration of care delivery, workforce support, continuity across settings, and robust governance. When these elements are aligned, health systems can respond to demand without compromising the human foundations of care.

Developed within this context, Precise Clinical brings these elements together through hybrid delivery, continuity-focused design, workforce-aware structures, and embedded clinical governance. The result is a care framework designed to sustain psychiatric services over time, even as pressures on the workforce continue to evolve.
Sources:
- Levin, E., & Aburub, H. (2024, April 22). Barriers and solutions to comprehensive care for mental health patients in hospital emergency departments. Journal of Mental Health & Clinical Psychology. https://www.mentalhealthjournal.org/articles/barriers-solutions-comprehensive-care-mental-health-patients-hospital-emergency-departments.html
- Xiong, B., Bailey, D. X., Stirling, C., Prudon, P., & Martin-Khan, M. (2025, December 2). Barriers, enablers, and impacts of implementing National Comprehensive Care Standards in acute care hospitals: An interview study. MDPI. https://www.mdpi.com/2039-4403/15/12/428
- Hernandez, V., Nasser, L., Do, C., & Lee, W.-C. (2024, August 22). Healing the whole: An international review of the collaborative care model between Primary Care and Psychiatry. MDPI. https://www.mdpi.com/2227-9032/12/16/1679
- Sipos, D., Goyal, R., & Zapata, T. (2024, June 11). Addressing burnout in the healthcare workforce: Current realities and mitigation strategies. The Lancet regional health. Europe. https://pmc.ncbi.nlm.nih.gov/articles/PMC11281910/
- Aggarwal, K., Singh, B., Banker, H., Stoltzfus, M. T., Hong, J., Anamika, F., Nishkamni, F., Munjal, J., & Jain, R. (2024, May 28). Exploring the ramifications of delayed hospital discharges: Impacts on patients, physicians, and Healthcare Systems. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC11210572/
- Gilles, I., Le Saux, C., Zuercher, E., Jubin, J., Roth, L., Bachmann, A. O., & Peytremann-Bridevaux, I. (2025, April 9). Work experiences of healthcare professionals in a shortage context: Analysis of open-ended comments in a Swiss cohort (SCOHPICA). BMC health services research. https://pmc.ncbi.nlm.nih.gov/articles/PMC11984188/
Written by Gabriella Aaron
About the Authors
Gabriella Aaron is a Clinical Research and Content Development Specialist at Precise Behavioral, Inc., with a background in Medical Microbiology and a passion for digital mental health solutions.
Editorial Contributors
This piece was edited by Greta Baker and Kirsten Guiliano.


